MDSteps gives IMGs full access to 16,000+ USMLE-style questions, 135 CCS cases, analytics, flashcards, visual rationales, and clinical reasoning tools without buying separate add-ons. Cancel anytime. First month protected by our 7-day good-faith refund guarantee after 100 questions or 5 CCS cases. Definition. ECFMG certification confirms that an IMG has passed USMLE Step 1 and Step 2 CK and satisfied the communication/clinical skills requirement, enabling entry into ACGME-accredited training and eligibility for Step 3. Because the discontinued clinical skills exam was replaced by Pathways, most candidates now complete the communication requirement via OET Medicine plus a qualifying Pathway. Macro-timeline. If you plan to submit ERAS in September, anchor backward: (1) Identity verification (Form 186 via NotaryCam in MyIntealth) → (2) EPIC portfolio & primary-source document verification → (3) USMLE sequencing (Step 1 then Step 2 CK, or reverse based on background and score needs) → (4) Pathway application & OET Medicine → (5) Final certificate issuance before residency start. Each component has its own processing time; start the “slow lanes” first and run the “fast lanes” in parallel. Critical dependencies. Your medical school must be listed in the World Directory of Medical Schools (WDOMS) with an ECFMG-eligible Sponsor Note for your graduation year; otherwise, you are not eligible to test under ECFMG sponsorship. Confirm this before spending money on exams. Milestone gating. You cannot schedule USMLE until your eligibility is confirmed and you receive a scheduling permit; Prometric access is then opened for available dates (often ≤6 months ahead). These gating points mean that a late Form 186 or missing transcript can push your whole plan by weeks. What “done” looks like. Certification is awarded when ECFMG confirms your exam passes and Pathway/OET requirements. Check if any prior, time-limited Pathway acceptance you relied on needs revalidation; some Pathways-based certificates can expire if not made valid indefinitely. MyIntealth account. All modern ECFMG services—including exam applications and EPIC—run through MyIntealth. Create your account early, confirm the name on your passport matches exactly, and add a secondary email for redundancy. This will also be your portal for payments and status checks across services. Form 186 (identity verification). The Certification of Identification (Form 186) is notarized online via NotaryCam using your valid passport. This single step gates almost everything else (exam applications, EPIC). Schedule notarization at a time you can be uninterrupted, test your video setup, and keep scans of passport/residency ID ready. Processing is generally quick but can vary; tackle it as your very first action item. Eligibility to test. Students require current enrollment that meets ECFMG criteria; graduates must hold a diploma from a WDOMS-listed school with an ECFMG Sponsor Note that includes their graduation year. If the Sponsor Note was updated, verify that your year remains covered; if it doesn’t, resolve with your registrar before applying. Practical setup. Use a consistent legal name across passport, MyIntealth, EPIC, and USMLE. Store notarized documents and receipts in a cloud folder. If your passport will expire within 6–9 months, renew it; a mid-process name/number change can trigger re-verification and delays. MDSteps tip. While identity steps process, spin up your MDSteps automatic study plan generator to map your hours to an eligibility period; it adapts to your calendar and produces an integrated to-do list (QBank blocks, review, spaced recall). Pair it with the Adaptive QBank (9,000+) and the readiness dashboard to watch predicted performance as you lock study windows. MDSteps helps you connect Steps 1–3, CCS, weak-area tracking, flashcards, and study planning in one workflow while you manage certification and Match pressure. What EPIC does. ECFMG’s EPIC service verifies your credentials directly with your medical school (primary-source verification). You’ll upload documents (diploma, transcripts), pay fees, and issue verification requests to your school. Intealth/ECFMG then contacts the school and records the primary-source response. Flawless document prep. Submit crisp, complete scans, including seals/stamps and backs of documents if they contain notations. If your diploma is not in English, provide a certified translation and upload both. Ensure the name on the diploma matches your passport (include official name-change proof if needed). Many “return for correction” cases are preventable—mismatched names, cropped seals, or incomplete pages are classic pitfalls. School coordination. Identify your registrar/records office contact and confirm their preferred channel (portal vs institutional email). Share your EPIC request numbers and ask about typical turnaround time. Some schools respond within days; others, weeks. Nudge politely every 10–14 days with your identifiers and a one-line summary of what’s pending. Rejections & remediation. If EPIC marks a document as “not acceptable,” fix what the note specifies. If a registrar refuses verification due to formatting or a missing stamp, request a reissue that EPIC will accept. Always keep a log: date submitted, EPIC ticket, school action, next step. It becomes invaluable if you escalate. Parallelism. Run EPIC in parallel with early exam prep. While you cannot control registrar speed, you can subtract risk by finishing OET/Pathway and exams on time. Your certification cannot be finalized until EPIC data align with exam results, so treat documents as a critical path. Sequence logic. Choose between (A) Step 1 → Step 2 CK if your basic-science foundation is strong and you want to establish momentum, or (B) Step 2 CK first if you’re a recent clinical graduate with strong wards exposure and need an earlier competitive score for ERAS. Either route can work; what matters is the calendar: pick eligibility periods that allow realistic prep (12–20 weeks each for most IMGs) and avoid overlapping with EPIC/OET crunch weeks. Eligibility periods & Prometric. You apply for an eligibility period, receive a scheduling permit, then book a seat on Prometric. Seats may not be open more than ~6 months out, and high-demand cities fill fast—especially near ERAS deadlines and holidays. If you can travel to a less busy center, you may gain 2–6 weeks of schedule control. Reschedules & contingencies. If your practice NBME/MDSteps assessments are below target two weeks out, rescheduling is often cheaper than risking a suboptimal score. Build a single “slip week” into each window. After you finish Step 1, pivot immediately to CK content while fundamentals are fresh. MDSteps integration. Use the Adaptive QBank (9,000+) in timed, mixed mode to build pattern recognition early; let the readiness dashboard guide eligibility period selection. Missed items auto-generate exportable flashcards for spaced retrieval (Anki-ready). The MDSteps Tutor can walk you through board-style reasoning when you’re stuck, but keep most practice in testing conditions. Why OET Medicine. For candidates using the Pathways, ECFMG requires a satisfactory OET Medicine performance across all four subtests (Listening, Reading, Writing, Speaking). There are no exemptions based on native language or language of instruction. Book a date that leaves buffer for a retake if needed, but aim to pass once. Scheduling for match-year timelines. For participation in a given NRMP Match, ECFMG historically advises completing OET Medicine early enough to allow score reporting and Pathways processing before the application deadline. Check the current cycle’s dates as you plan, then place OET far enough in advance that a contingency retake still fits. Passing on the first try. Treat OET like a clinical communication OSCE: rehearse introductions, signposting, empathy, and agenda-setting; master the referral/discharge letter format; and practice timing. Build a 4–6 week micro-plan: two speaking role-plays per day, daily reading/listening sets, and twice-weekly timed writing tasks with rubric-based feedback. Use transcript-to-talkback: record, transcribe, and correct. Integrating with USMLE prep. Block 45–60 minutes per day during lighter USMLE weeks for OET skills; this reduces cognitive interference and avoids last-minute cramming. If writing is your weak area, front-load additional sessions because its feedback loop is slower. Evidence-informed drills. Chunk speaking into micro-skills (openings, agenda, ICE—ideas/concerns/expectations, teach-back) and practice with time pressure. For writing, build phrasebanks for diagnosis/plan/justification statements and rehearse visually (e.g., standard paragraph scaffolds). Finish with two full mocks at exam timing. What Pathways solve. Pathways replace the old clinical skills exam by validating your clinical/communication readiness through specified criteria. The right Pathway depends on your licensure status, school accreditation/attestations, and recent supervised practice. Start with ECFMG’s official Pathways overview, then map your facts to the decision tree. Fast matching. If you have a recent unsupervised license/registration, examine Pathway 1; if not, review the school-based or practice-based Pathways applicable to your situation. Prepare proofs (license letters, supervised practice attestations) and confirm that names, dates, and license numbers align across documents. Cycle-specific deadlines. Deadlines and window guidance (e.g., last OET test dates; Pathways application cutoff) vary by year. Missing them jeopardizes participation in that Match cycle. Set calendar reminders upon release of the new cycle page, and submit early to allow for correction loops. Expiration & revalidation. If your prior Pathway acceptance or certificate was time-limited, confirm whether it expires and whether revalidation is needed before residency start or Step 3. Planning to rely on an older acceptance without checking status is a dangerous assumption. MDSteps alignment. As soon as you lock your Pathway and OET date, use the MDSteps study plan generator to adjust your USMLE cadence. The platform’s readiness dashboard helps you decide whether to take CK earlier for ERAS leverage or later for score maximization, while auto-generated flashcards compress facts efficiently. Fees & budgeting. Expect separate fees for exam registrations (Step 1/CK), EPIC services, OET Medicine, and notarization (NotaryCam). ECFMG and USMLE publish current fees annually; build a buffer for rescheduling and additional document requests. Check the current fee page and your cycle’s information booklet before paying. Scheduling mechanics. After eligibility is approved, you’ll receive a scheduling permit; book at Prometric and watch for seat releases (often within a ≤6-month window). Use calendar holds for 2–3 potential test dates to absorb life events without derailing the timeline. Score timing & ERAS. Typical score releases occur on Wednesdays, with occasional delays around major holidays or maintenance windows. Build in 3–4 weeks after test day before you expect official results, then add time for processing and certificate issuance (once all other requirements are met). When in doubt, take exams earlier rather than later to avoid missing ERAS milestones. Step 3 strategy (optional pre-residency). Some IMGs take Step 3 before Match to strengthen applications or meet certain visa/state nuances. If you choose this, plan a short ramp after CK to focus on management, ethics, and biostatistics. For case practice, MDSteps offers live-vitals CCS Cases with timed orders and physiologic responses—useful if you elect an early Step 3 run. Confirm current Step 3 fees and eligibility directly with FSMB. High-level planning. Assume a 20-week run-up to ERAS with parallel lanes. Weeks 1–2: MyIntealth, Form 186, EPIC portfolio creation, registrar outreach; configure MDSteps plan and baseline assessment. Weeks 3–10: Step 1 or CK primary prep; weekly mixed timed blocks; start OET micro-drills (20–30 minutes/day). Weeks 11–16: Second exam block prep; file Pathway application as soon as documents are ready; keep EPIC corrections moving. Weeks 17–18: Sit first exam (if not already); intensify OET speaking/writing mocks. Weeks 19–20: Sit second exam; complete OET; ensure EPIC verifications complete; verify certificate status and ERAS uploads. Mini-algorithm for sequencing. If your basic science is ≥ready and your ERAS strategy benefits from early score visibility, take Step 1 first; if you graduated recently and your clinical pattern recognition is stronger, take CK first. In both cases, lock eligibility periods that leave one slip week and position score release ≥4 weeks before your ERAS target date. Why this works. By front-loading slow administrative items (identity, EPIC) and building exam/OET lanes in parallel, you reduce the risk of a single bottleneck spoiling a cycle. Using data-informed readiness from MDSteps to pick eligibility periods keeps your plan realistic and resilient—even if a registrar needs an extra week or a Prometric seat shifts by a few days.One $27/month subscription for Step 1, Step 2 CK, Step 3, and CCS.
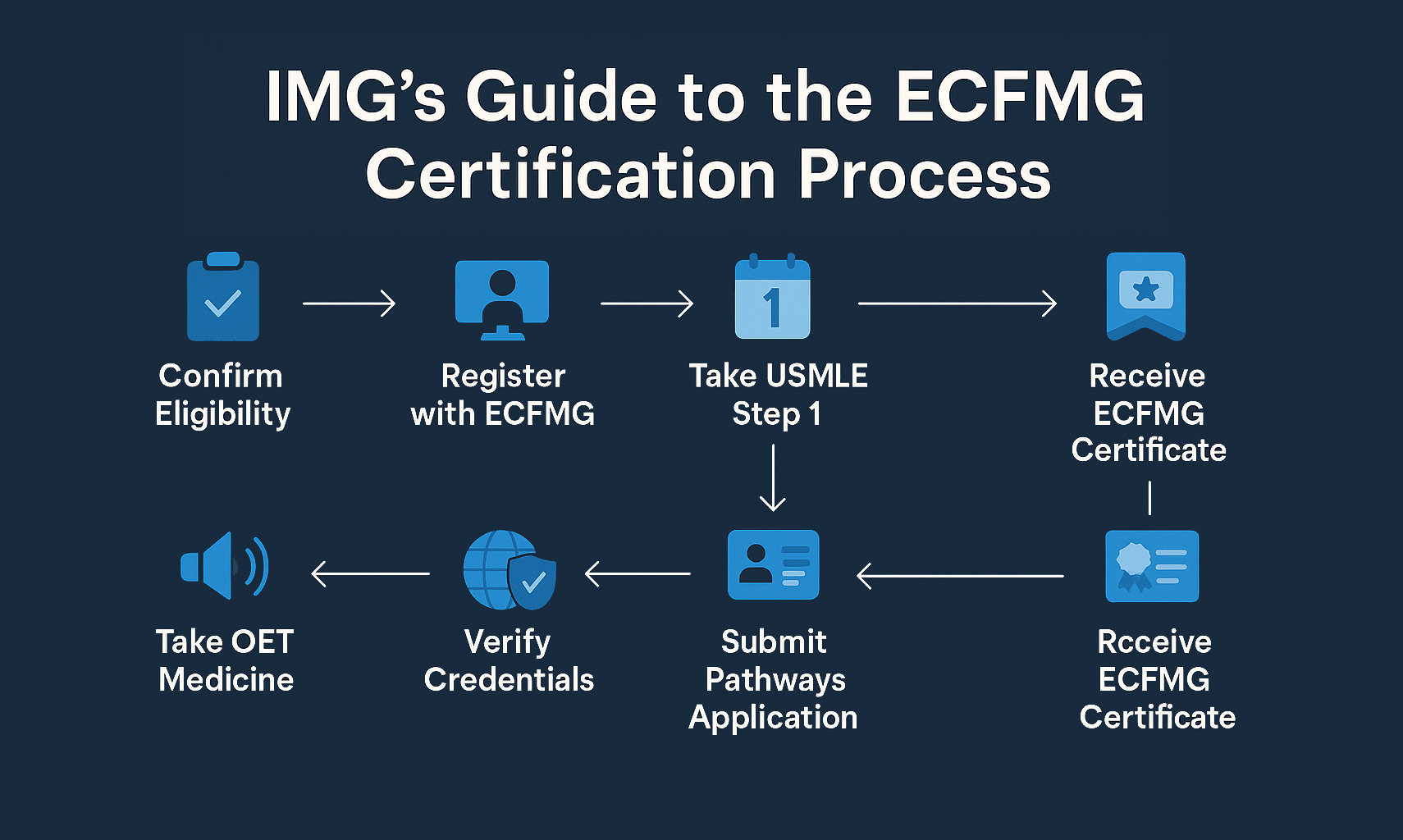
Part 1 — The End-to-End Roadmap: What “Certified” Really Means
Part 2 — Identity & Eligibility: MyIntealth, Form 186, and WDOMS
IMG prep gets harder when every requirement lives in a different tool.
Still missing questions you thought you understood?
Part 3 — EPIC & Primary-Source Verification: Zero-Mistake Workflow
EPIC Stage Owner Common Pitfall Prevention Portfolio setup Candidate Name mismatch vs passport Match passport exactly; attach name-change proof Document upload Candidate Cropped seals; missing back page Scan all sides; 300+ dpi; check legibility Verification request EPIC→School Registrar unresponsive Confirm contact; calendar gentle nudges q10–14d Correction loop Candidate Wrong translation format Use certified translator; upload original + translation Part 4 — USMLE Sequencing & Scheduling: Windows, Centers, and Score Timing
Prep Length Weekly Structure (MDSteps) Target Blocks/Week Checkpoint 12 weeks 5 study days + 1 review + 1 rest 14–18 timed tutor→timed exam Week 6 diagnostic; adjust plan 16 weeks 5–6 study days + 1 review 18–22 mixed timed blocks Week 8 midpoint readiness 20 weeks 6 study days + rolling review 22–26 mixed timed blocks Week 10 full-length Part 5 — OET Medicine: Meeting the Communication Requirement Without Re-Testing
Part 6 — Pathways Selection: Choose Correctly in Minutes
Part 7 — Costs, Logistics, and Score Release: Budgeting Time and Money
Category Typical Items Notes Identity Form 186 via NotaryCam Use valid passport; schedule early Exams Step 1, Step 2 CK Separate fees per exam; reschedule fees apply EPIC Portfolio + verification requests Fees per document; registrar timelines vary OET OET Medicine test Book with retake buffer; all four subtests required Travel Prometric center costs Consider off-peak cities for availability Part 8 — Putting It Together: 20-Week Master Plan + Rapid-Review Checklist
Rapid-Review Checklist
Frequently Asked Questions (IMG → ECFMG Certification)
References & Official Resources
ECFMG & Intealth
ECFMG Certification for IMGs: Step-by-Step Roadmap
For IMG exam planning
Requirements tell you what is due. Practice data tells you what is weak.
Use MDSteps to turn your IMG timeline into targeted question blocks, weak-area repair, CCS practice, and readiness signals.
Full access includes Step 1, Step 2 CK, Step 3, CCS cases, analytics, auto-flashcards, and study planning.
Pivot-clue review
See the exact phrase in the stem that should have changed your decision.
Distractor trap logic
Learn why the answer you almost picked felt right—and why it was wrong for this patient right now.
Miss-pattern analytics
Turn repeated mistakes into targeted blocks, flashcards, and readiness signals.
Quick Take: ECFMG certification requires two pillars—passing USMLE Step 1 and Step 2 CK, plus meeting the communication/clinical skills requirement (typically via Pathways + OET Medicine). Build your sequence backward from ERAS deadlines, and remove bottlenecks early (Form 186 identity verification, EPIC document workflow, and test-center scheduling).
Affordable USMLE Prep for IMGs
Score stuck after more questions?
Free reasoning diagnostic
Pivot clue isolatedDistractor trap explainedNext study target identified
No credit card required for the free reasoning review. Full access is $27/month after that. Cancel anytime.
Reasoning diagnostic
Still missing the same kinds of questions?
Read why that happens.
Most IMGs who plan proactively complete identity (Form 186) and EPIC setup in 2–6 weeks, then finish USMLE Step 1 + Step 2 CK in 6–10 months depending on baseline. OET Medicine and Pathways can be completed in parallel (4–8 weeks). Final certificate posting follows after all components are satisfied. Build buffers for registrar delays and test-center availability.
EPIC is Intealth’s primary-source verification service for your credentials (e.g., diploma, transcript). ECFMG certification requires passing Step 1 and Step 2 CK plus meeting the communication/clinical skills requirement (Pathways + OET Medicine). EPIC feeds verified documents into your ECFMG file; exams and Pathways are separate.
Eligibility hinges on your school’s WDOMS entry and Sponsor Note for your graduation year. If a revision removed coverage for your year, resolve with your registrar or ECFMG before applying for USMLE eligibility. Keep a record (screenshot) of the exact wording.
No. Many IMGs with strong recent clinical exposure take CK first to secure an early, competitive score for ERAS. Others start with Step 1 to solidify foundations. Choose based on readiness and deadlines. MDSteps’ readiness dashboard can help forecast timelines and select eligibility periods.
You can retake OET Medicine as needed, but aim for one-and-done. ECFMG evaluates all four subtests; you must meet the published thresholds in each. Schedule early enough that a retake (if needed) still fits before Pathways deadlines.
Match your background to the official criteria: recent license/registration (Pathway 1), school-based attestations, supervised practice, or other specific conditions. Collect proofs and ensure dates and names align across documents. If eligible for more than one, favor the path with the clearest documentation and fastest turnaround.
Extensions and reschedules are possible but fee-bound and policy-limited. Check your permit for exact dates. Seats at Prometric are dynamic; consider a backup date in a secondary center and budget for one “slip week” per exam.
Possibly. Keep exactly the same legal name across passport, MyIntealth, EPIC, USMLE, and OET. If a change occurs mid-process, submit official documentation promptly and expect additional verification time. Renew an expiring passport early.
Identify a registrar contact, share EPIC request numbers, and follow up every 10–14 days with a concise note and identifiers. Keep a dated log. In parallel, progress OET, Pathways, and USMLE so certification isn’t bottlenecked by a single lane.
Optional. Some programs value a strong Step 3 for visa or state-specific reasons, but it isn’t universal. If you pursue it early, plan a focused post-CK block (management, ethics, biostatistics) and use MDSteps’ live-vitals CCS Cases to rehearse timed orders and physiology.
Yes. Upload the original and a certified translation that meets EPIC standards. Many rejections arise from incomplete pages or missing seals—scan both sides and verify legibility at 300+ dpi or higher.
Plan for EPIC portfolio and verification requests (per document), OET Medicine, notarization (NotaryCam) for Form 186, potential reschedule/extension fees, and travel to Prometric. Check the current official fee pages and add a 10–15% contingency.
Yes—USMLE is offered internationally at approved Prometric centers. Location does not alter scoring or validity. Practical considerations include seat availability, travel time, and costs. Some regions fill quickly near ERAS deadlines.
ECFMG certification itself is generally valid indefinitely once issued. However, some legacy Pathways acceptances were time-limited in past cycles. If you relied on an earlier Pathways approval, verify whether revalidation is needed before residency start or Step 3.
Pro tip: Use the MDSteps Automatic Study Plan Generator to align your USMLE windows with OET and Pathways milestones, and the Adaptive QBank + exportable flashcards to compress review as deadlines approach.