Why a 30-Day Plan Works on Rotations: Constraints, KPIs, and Guardrails
Thirty days is long enough to build pattern recognition and short enough to maintain intensity on service. The goal isn’t encyclopedic coverage; it’s decision speed on common inpatient and ambulatory problems. We anchor the month to three KPIs: question throughput (≥1,200 mixed clinical vignettes), retention yield (measured via spaced “hot list” items mastered), and readiness trend (practice-form trajectory with realistic confidence bands). These KPIs map to learning-science pillars: the testing effect (retrieval trumps reread), spaced repetition (durable memory with short, frequent passes), and interleaving (mixed domains sharpen discrimination under time pressure).
Rotations add constraints: post-call fatigue, pages, unpredictable procedures, and documentation. Therefore, the plan is built around time-boxed sessions you can deploy in 20–40 minute windows and a nightly rapid review that tops out at 25–30 minutes. We also enforce Friday slack—a built-in 10–15% buffer for life and service volatility—so the schedule doesn’t collapse after one bad week. Finally, we avoid cognitive overload by separating performance (timed blocks) from deliberate practice (slow, mechanism-first review) and by using a standardized error script so difficult cases convert into rules you’ll apply on exam day.
- Daily floor: 40–60 mixed questions (timed), even post-call (minimum 20).
- Review cap: 90 minutes on full days; 30 minutes post-call; defer deep dives to weekend.
- Practice cadence: diagnostic on Day 1 (baseline), progress check on Day 14, decision check on Day 24, dress rehearsal on Day 27.
- MDSteps tools: KPI tracker, incorrects pipeline, and rapid-review checklist templates embedded below.
Your job is to protect the floor, respect the caps, and let the pipeline do the compounding.
Calendar Architecture: Four Weeks That Survive Call and Clinic
Design the month like a service schedule: heavy weekdays, light post-call, strategic weekends. Each weekday has a core block (timed questions) before or after your shift, a micro-block you can do on your phone (2–4 rapid cards), and a review block at home. Weekends run longer, integrating deep review and a mixed diagnostic set. The sequence repeats across four weeks with slightly different emphasis (breadth → weakness targeting → consolidation → taper).
| Week | Focus | Weekday Target | Post-Call Target | Weekend Target | Outcome Metric |
|---|---|---|---|---|---|
| 1 (Days 1–7) | Breadth + Baseline | 40–60 Q/day (timed) | 20–30 Q + 20-min review | 120–160 Q + baseline review | Baseline score; initial hot list |
| 2 (Days 8–14) | Weakness Surfacing | 60 Q/day | 30 Q + tagged incorrects | 160–200 Q + systems pass | Midpoint check (Days 13–14) |
| 3 (Days 15–21) | Mechanism & Rules | 60–80 Q/day | 30 Q + rule-writing | 200 Q + algorithm drills | Rule bank >= 60 entries |
| 4 (Days 22–30) | Refine & Taper | 40–60 Q/day | 20–30 Q + rapid cards | Dress rehearsal + light review | Stable prediction interval |
Place practice forms on Days 1, 14, 24, and 27. Day 1 calibrates; Day 14 verifies slope; Day 24 informs the final 72-hour plan; Day 27 is a dress rehearsal with exam-day settings (breaks, pacing, nutrition). Build Friday slack by scheduling 10–15% fewer questions than your ceiling; use that space to catch up or to protect recovery after tough calls. If you miss a target, never raid sleep; redistribute into Friday or Saturday morning.
Daily Engine: Mixed Timed Blocks + a Tight Incorrects Workflow
The highest ROI comes from mixed, exam-length blocks under time pressure. Run 40–60 questions in timed mode (no tutor) with 90–105 seconds per item. Immediately after, execute a two-stage review. Stage A (fast): mark only items with diagnostic value—true uncertainty, lucky guesses, and conceptual misses—then log the why (knowledge gap, misread, premature closure, or anchoring). Stage B (deep): for the 8–12 most instructive items, write a one-sentence decision rule (e.g., “In painless jaundice + Courvoisier sign, next step is contrast CT for pancreatic head mass”). Convert that rule into a flashcard prompt (question stem fragment → next best step) and tag it by system and error type in your MDSteps incorrects pipeline.
MDSteps Incorrects Script (10–12 min)
- Classify error: knowledge vs. reasoning vs. attention.
- Extract trigger phrase(s) from the stem.
- Write the decision rule (if/then, next best step).
- Link mechanism (1–2 lines) to the rule.
- Create a review card & schedule spaced revisit.
Time Caps That Prevent Slog
- Weekdays: 60–90 min review cap per full block.
- Post-call: 20–30 min max; defer deep dives.
- Weekend: 2× depth on top 10 misses.
Avoid “museum tours” of explanations. Chase transfer: Would your rule change the next similar question? If yes, keep it. If not, archive it. When fatigued, prioritize next-step and management ladder items over esoterica.
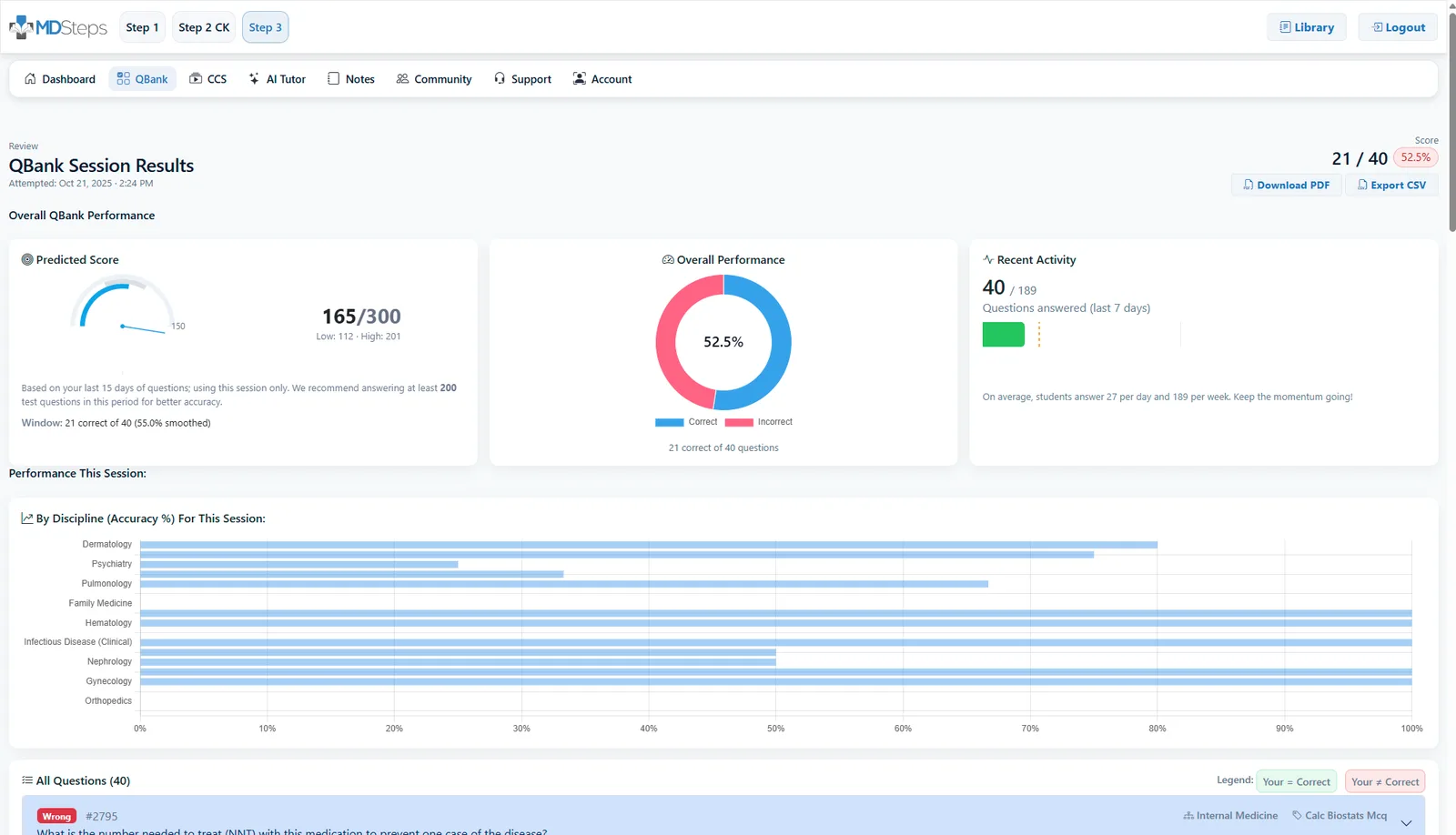
Learn the patterns behind your misses. Break the plateau.
If you keep narrowing stems to two answers and picking the distractor, the problem may not be your medical knowledge. MDSteps shows the pivot clue, the trap answer, and the reasoning pattern behind the miss—then turns it into targeted practice.
Still missing questions you thought you understood?
- Find the clue that should have changed your answer
- See why the distractor felt right
- Turn repeated misses into targeted practice
Content Consolidation: Rapid Review That Actually Finishes
On busy services, note bloat kills momentum. Consolidation should be brief, structured, and scheduled. Use a three-layer system: (1) Rules (your one-liners from incorrects), (2) Algorithms (management ladders for chest pain, GI bleed, stroke, sepsis, prenatal care), and (3) Microfacts (tight numeric anchors like Na⁺ correction rates, steroid stress-dose thresholds, or GAD-7 cutoffs). Your nightly rapid review cycles 6–10 rules, 1–2 algorithms, and 6–10 microfacts in 25–30 minutes.
MDSteps Rapid Review Pipeline (25–30 min cap)
- 5 min: Resurface yesterday’s “due” rules (spacing).
- 10–15 min: New rules from today’s blocks (interleaved).
- 5–7 min: One algorithm rehearsal (say-it-out-loud steps).
- 2–3 min: Microfacts lightning round (numeric anchors only).
Tip: Keep cards terse and recognition-proof. Stem fragment → action. Ditch paragraphs; use verbs and thresholds.
Weekend consolidation adds a systems pass without abandoning interleaving. Do a 60–90 minute walk-through of the highest-weight domains (medicine, OB/GYN, pediatrics, surgery, psychiatry) using mixed question sets to surface blind spots, then plug them into the rule bank. Resist the urge to build encyclopedias; the exam rewards pattern + next step more than trivia. Finally, track leakage—the handful of rules you repeatedly miss. Give them double spacing and rehearse with oral recall to ensure generative retrieval, not recognition.
Diagnostics & Decision-Making: Turning Practice Scores into Action
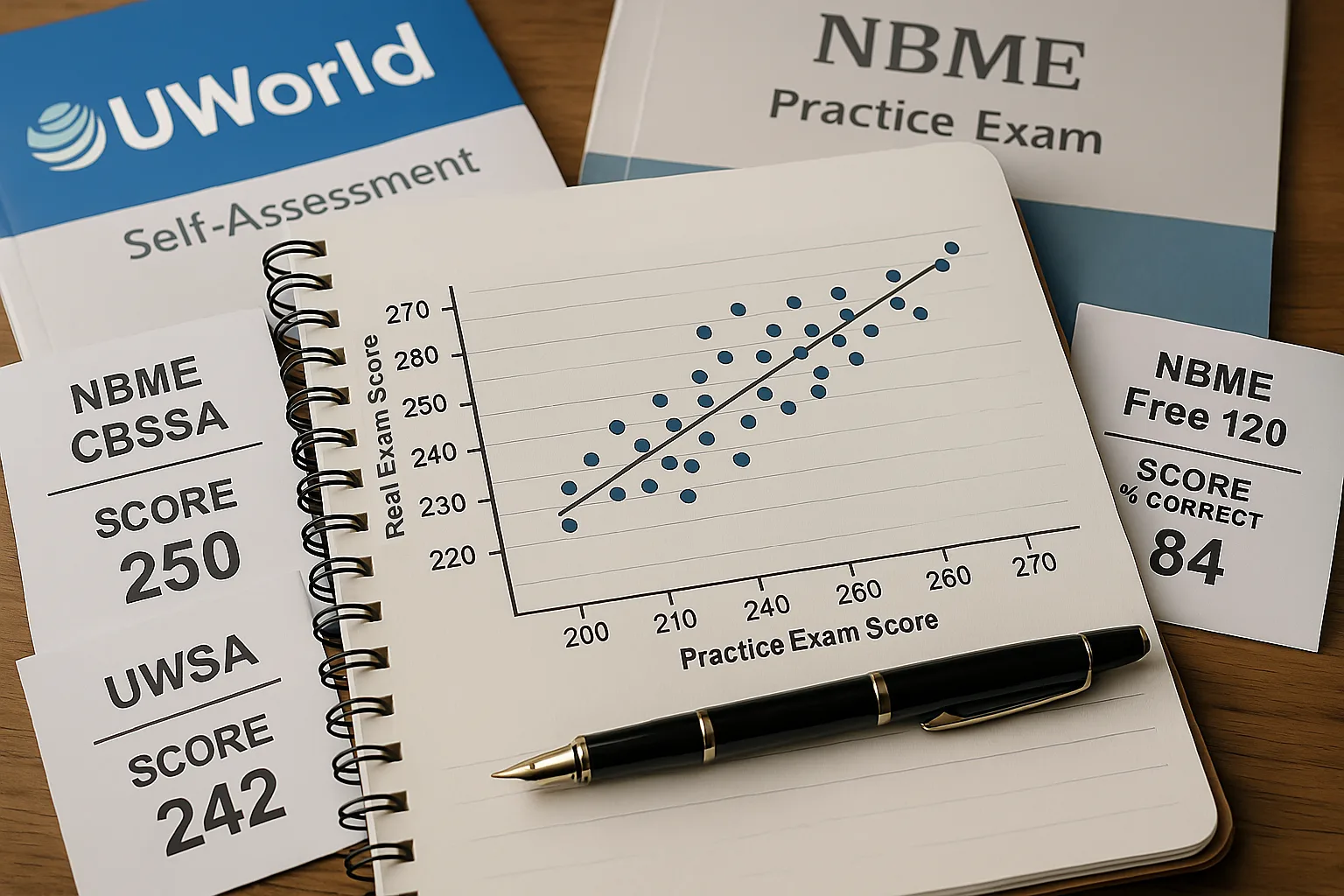
Practice forms are instruments, not verdicts. Each carries both signal (your current level) and error (form difficulty, test-day variance). Treat every result as a range, not a point. Compute a conservative prediction interval by subtracting 5–8 points from your form score to define a floor for planning; if multiple forms cluster, weight the median. Look beyond the total: domain bands (e.g., cardiovascular, respiratory, renal), task types (diagnosis, next step, ethics), and error taxonomy (knowledge vs reasoning vs attention) dictate the next 72 hours of work.
Score → Action Framework
- Baseline (Day 1): Set starting range; identify 3 weak domains.
- Midpoint (Day 14): Check slope. If flat or negative, trim passive reading and add a second mixed block daily for five days.
- Pre-decision (Day 24): If your conservative floor is at or above your target band, proceed; if not, add a 7–10 day micro-extension focused on the top two deficits.
- Dress rehearsal (Day 27): Simulate breaks and pacing; finalize logistics and nutrition plan.
Interpretation note: Consistency across forms beats one high flyer. Outliers are often noise.
Common Pattern Flags
- Low diagnosis, normal management: Add differential drills with triage cues.
- Normal diagnosis, low next step: Rehearse algorithms aloud; build ladder cards.
- High omissions/marked items: Work on pacing (90-sec rule) and first-pass elimination.
Finally, make domain sprints tiny and tactical (e.g., “OB third-trimester bleeding: 30 mixed questions + 3 rules + 1 algorithm”). Ship outcomes within 24 hours, then return to mixed sets to protect transfer.
What to Study First: High-Yield Domains and How to Weight Them
Step 2 CK emphasizes common inpatient and ambulatory scenarios where recognition and management speed matter. Rather than chasing exact percentages (which fluctuate across forms), anchor your time to a pragmatic weighting: Internal Medicine (broad adult care) as the backbone; OB/GYN and Pediatrics for age- and pregnancy-specific algorithms; Surgery for perioperative and trauma management; and Psychiatry/Ethics for safety, capacity, and consent. Within each, prioritize next best step ladders, red-flag triage, and numeric thresholds likely to change management.
| Domain | Pragmatic Emphasis | Core Algorithms to Rehearse | Numeric Anchors |
|---|---|---|---|
| Internal Medicine | High | Chest pain, GI bleed, DKA/HHS, sepsis bundle, AKI | Troponin deltas, MELD/Child-Pugh cues, MAP goals, Na⁺ correction |
| OB/GYN | Moderate-High | Third-trimester bleeding, hypertensive disorders, labor management | Severe-feature BPs, MgSO₄ dosing, RhIg timing |
| Pediatrics | Moderate | Fever in <28/29–60/61–90 days, asthma exacerbation, dehydration | Weight-based fluids, bronchodilator escalation, bilirubin thresholds |
| Surgery/Emergency | Moderate | Abdominal pain triage, trauma primary survey, periop abx/anticoag | Transfusion triggers, hemodynamic targets, NPO windows |
| Psychiatry/Ethics | Moderate | Suicide risk, capacity, involuntary hold, confidentiality exceptions | Screen thresholds (e.g., PHQ-9 bands), criteria snippets |
Spend the first 10 days slightly overweighting Internal Medicine while keeping daily interleaving across OB/GYN, Pediatrics, Surgery, and Psychiatry to maintain discrimination. As weaknesses surface, reallocate 20–30% of daily volume toward those domains for three-day sprints, then return to mixed blocks. Keep a living Numeric Anchors card list; the step from “consider” to “do” often hinges on a range or cutoff.
On-Service Tactics: Studying Through Fatigue, Call, and Clinic
Clinical days drain willpower; design friction-proof habits. Morning micro-set: 6–8 questions on your commute or pre-rounds coffee to prime retrieval. Mid-day reset: if you get 10 minutes, rehearse 3–5 rule cards, not social media. Post-call protocol: 20–30 mixed questions (timed) to keep rhythm, 20-minute rapid review, then full recovery—no guilt. Protect sleep like a medication with strict dosing and timing; the testing effect collapses without consolidation.
Pacing & Error-Proofing on Timed Blocks
- 90-second rule: If you’re stuck, mark, eliminate obvious distractors, pick the leading hypothesis, move on.
- Red-flag first: Vital instability or airway threat? Choose stabilization before diagnostics.
- Read the last line first: Clarifies the task (diagnosis vs. next step vs. test choice) and prevents explanation tours.
- One-pass elimination: Kill answers that violate the stem’s facts or the algorithm’s sequence.
Use the ward to your advantage. When you encounter a case (e.g., pancreatitis, UGIB, preeclampsia), write a 48-hour mini-sprint: 20 related questions, 3 decision rules, 1 algorithm rehearsal. Discuss the ladder with a senior or attending to sharpen pragmatics. For documentation-heavy days, switch to micro-blocks: three 7-question bursts spaced through the day behave like one 21-question set and keep your streak intact. Finally, prevent erosion by setting a daily shutdown ritual (screen off, tomorrow’s question count set, three wins noted). Momentum beats motivation.
Final 72 Hours, Exam-Day Logistics, and the Rapid-Review Checklist
The last three days convert knowledge into execution. Day −3: two mixed blocks (timed), 60–90 minutes of targeted review, algorithm rehearsal aloud, finalize travel and ID. Day −2: one full mixed block plus a light incorrects sweep; confirm meals, fluids, layers, and break structure. Day −1: half-day only—one 40-question set, 20-minute rapid cards, and a walk; screens off by 7–8 p.m., sleep on schedule. If anxiety spikes, rehearse your first 10 minutes—check-in, locker, earplugs, first passage cadence.
Rapid-Review Checklist (Print or Save)
- Top 30 decision rules (cardiac chest pain, stroke window, sepsis bundle, GIB ladder, DKA/HHS, third-trimester bleed, neonatal fever).
- 10 algorithms said aloud (no notes): ACS, PE, COPD/Asthma exacerbation, AKI, prenatal care by trimester, hypertensive disorders of pregnancy, pediatric fever age-bands, suicide risk, delirium vs dementia, perioperative anticoagulation.
- Numeric anchors: insulin infusion starts, MgSO₄ dosing, Na⁺ correction rates, transfusion triggers, steroid stress dosing, bilirubin phototherapy thresholds.
- Pacing: 90–100 seconds per item with a planned second sweep for marked questions.
- Break plan: fluids every two blocks, protein + complex carbs, brief stretch, eye rest.
- Logistics: ID, confirmation, earplugs/headphones, layers, simple snacks, charged ID-approved calculator if allowed.
Mindset cue: The exam is a sequence of solvable vignettes. Execute your routine, trust your rules, and keep moving.
References & Further Reading
- USMLE®. Prepare for Your Exam (exam structure, content outline, timing).
- NBME®. Practice & Self-Assessment (forms and score interpretation resources).
- Cepeda NJ, Pashler H, Vul E, et al. Distributed practice in verbal recall tasks. Psychol Sci. 2006. (Spacing effect).
- Roediger HL, Karpicke JD. Test-enhanced learning. J Educ Psychol. 2006. (Testing effect).
- Sweller J. Cognitive load during problem solving. Cogn Sci. 1988. (Cognitive load theory).
- Taylor K, Rohrer D. The effects of interleaving. Appl Cogn Psychol. 2010. (Interleaving benefits).